The lasting impact of the Covid crisis on economic potential.
As the global economy recovers from the immediate economic impact of the Covid crisis, attention is increasingly turning to the long-run impact of the shock on productivity. This column identifies several channels – including labour market hysteresis, impaired skill acquisition, belief scarring, an increase in zombie companies, and policy errors – through which the lasting harm will outweigh any positive supply shocks caused by the pandemic. The authors estimate long-term output losses in the order of 3% of global GDP. Scarring will be greater in some economies than others, pointing to the importance of policy in mediating and offsetting these channels.


Canada: no change
Trudeau may be back in office, but like the other G7 economies, things are not rosy economically. Canada’s 2021 economic outlook is similar to that of other developed countries. After the largest economic contraction since 1945 (a dip of 5.5% of GDP in 2020), Canada is still in recession, according to the latest figures, although forecasters (Oxford Economics) are still expecting a sharp recovery.

…
So the decade since 2009 has been characterized by sneaking stagnation, rooted in profitability problems that began after 2005. This has manifested itself in the stagnant accumulation of machinery and equipment, low industrial capacity utilization rates, low employment levels, as well as low real wage and GDP growth. It is an expression of what I have called the Long Depression that all the major capitalist economies have sunk into since 2009 in the ten years leading up to the COVID slump.
And just as in other major G7 economies, corporate and household debt has jumped to record highs.
… The Bank of Canada economists have classified 25% of Canada’s publicly traded companies as zombie firms ie. they persistently do not earn enough revenue to cover interest payments on their outstanding debts.
So Canadian capitalism bears all the hallmarks of the contradictions facing the rest of the G7 economies as they come out of the COVID slump. PM Trudeau achieved nothing with his snap election and faces the same problems in getting Canada’s capitalist economy going as before.
The Fed, interest rates and stagflation
So even if ‘quantitative easing’ begins to tail off next year, interest rates will stay very low or near zero for at least another year. The Fed is in a quandary. Low interest rates are bad because too much borrowing at cheap rates could lead to higher and sustained inflation if supply cannot match accelerating demand, while borrowing for speculation in financial assets and property will continue. On the other hand, hiking interest rates will raise the cost of servicing existing debt, now at record levels, which could eventually lead to defaults, bankruptcies and a financial crash. The Fed is not sure which way to go.
But then neither is mainstream economics. That’s partly because mainstream economics has no clear explanation for low interest rates. The neo-classical/Austrian view is that market interest rates depend on the supply and demand for savings and investment. When the former is higher than the latter, interest rates will fall to reach a new equilibrium. This is called the natural rate of interest or r*. The Austrian school adds that if the central bank intervenes in this market for capital by pumping in money credit, it distorts the market rate below the natural rate which will eventually lead to a credit crunch. And this is what is happening now.
But is there a natural rate of interest? Does this concept help us understand what is happening in an economy, especially in the major capitalist economies, right now? Keynes dismissed the idea arguing that there was not one static natural rate but a series of rates depending on the level of investment, consumption and saving in an economy and the desire to hoard money (liquidity preference). There was no reason to assume that the capitalist economy would ‘correct’ any mismatch between investment and savings, particularly in a depression, by market interest rates adjusting back to the ‘natural rate’ in some automatic market process. That’s because in a depression where investment returns are too low compared to the money rate of interest, capitalists will hoard their money rather than invest in a ‘liquidity trap’.
Both Keynes and Marx looked not to a concept of a natural rate of interest’ but to the relation of interest rate for holding money to the profitability (or return) on productive capital. Actually, so did the author of the natural rate, Wicksell. According to Wicksell, the natural rate is “never high or low in itself, but only in relation to the profit which people can make with the money in their hands, and this, of course, varies.
…
The post-Keynesian thesis is to argue that interest rates reach lows because savings outstrips spending. It’s households that start to hoard money rather than spend. One explanation for this up to now has been based on demographics; namely the older people tend to spend less and save more – and everywhere the advanced capitalist economies are aging. However, the latest explanation is that it is rising inequality that is a creating a ‘savings glut’ because richer people tend to save more than poorer people. This is an argument that has been presented for some time, particularly on an international plane, where Keynesians have argued that there has been a ‘global savings glut’ in trade surplus countries like China, Japan or Germany and their surplus capital has been transferred into the US, driving down interest rates.
…
There is no global or national ‘savings glut’. Instead the problem is an ‘investment dearth’.
…
In my view, low interest rates are not the result of a lack of aggregate demand caused by rising inequality and the inability of workers to buy back their own production. It is the result of the declining profitability of capital in the major capitalist economies
…
Accelerating inflation may be an issue right now in the US and other recovering capitalist economies, and it certainly bites into any recovery in labour incomes; but for capitalism, profitability is the real benchmark and that can be hit by wage rises on the one hand and interest rises on the other. If it is, that is the basis for a new slump.
Pettis: Are We Starting to See Why It’s Really the Exorbitant “Burden”
The role of the U.S. dollar as the world’s global reserve currency has been regarded as a great advantage to the United States but actually it is a destabilizing burden rather than an “exorbitant privilege.”
The Global Housing Market Is Broken, and It’s Dividing Entire Countries
The dream of owning a home is increasingly out of reach. Democratic and authoritarian governments alike are struggling with the consequences.
So the decade since 2009 has been characterized by sneaking stagnation, rooted in profitability problems that began after 2005. This has manifested itself in the stagnant accumulation of machinery and equipment, low industrial capacity utilization rates, low employment levels, as well as low real wage and GDP growth. It is an expression of what I have called the Long Depression that all the major capitalist economies have sunk into since 2009 in the ten years leading up to the COVID slump.
And just as in other major G7 economies, corporate and household debt has jumped to record highs.
… The Bank of Canada economists have classified 25% of Canada’s publicly traded companies as zombie firms ie. they persistently do not earn enough revenue to cover interest payments on their outstanding debts.
So Canadian capitalism bears all the hallmarks of the contradictions facing the rest of the G7 economies as they come out of the COVID slump. PM Trudeau achieved nothing with his snap election and faces the same problems in getting Canada’s capitalist economy going as before.
The Fed, interest rates and stagflation
So even if ‘quantitative easing’ begins to tail off next year, interest rates will stay very low or near zero for at least another year. The Fed is in a quandary. Low interest rates are bad because too much borrowing at cheap rates could lead to higher and sustained inflation if supply cannot match accelerating demand, while borrowing for speculation in financial assets and property will continue. On the other hand, hiking interest rates will raise the cost of servicing existing debt, now at record levels, which could eventually lead to defaults, bankruptcies and a financial crash. The Fed is not sure which way to go.
But then neither is mainstream economics. That’s partly because mainstream economics has no clear explanation for low interest rates. The neo-classical/Austrian view is that market interest rates depend on the supply and demand for savings and investment. When the former is higher than the latter, interest rates will fall to reach a new equilibrium. This is called the natural rate of interest or r*. The Austrian school adds that if the central bank intervenes in this market for capital by pumping in money credit, it distorts the market rate below the natural rate which will eventually lead to a credit crunch. And this is what is happening now.
But is there a natural rate of interest? Does this concept help us understand what is happening in an economy, especially in the major capitalist economies, right now? Keynes dismissed the idea arguing that there was not one static natural rate but a series of rates depending on the level of investment, consumption and saving in an economy and the desire to hoard money (liquidity preference). There was no reason to assume that the capitalist economy would ‘correct’ any mismatch between investment and savings, particularly in a depression, by market interest rates adjusting back to the ‘natural rate’ in some automatic market process. That’s because in a depression where investment returns are too low compared to the money rate of interest, capitalists will hoard their money rather than invest in a ‘liquidity trap’.
Both Keynes and Marx looked not to a concept of a natural rate of interest’ but to the relation of interest rate for holding money to the profitability (or return) on productive capital. Actually, so did the author of the natural rate, Wicksell. According to Wicksell, the natural rate is “never high or low in itself, but only in relation to the profit which people can make with the money in their hands, and this, of course, varies.
…
The post-Keynesian thesis is to argue that interest rates reach lows because savings outstrips spending. It’s households that start to hoard money rather than spend. One explanation for this up to now has been based on demographics; namely the older people tend to spend less and save more – and everywhere the advanced capitalist economies are aging. However, the latest explanation is that it is rising inequality that is a creating a ‘savings glut’ because richer people tend to save more than poorer people. This is an argument that has been presented for some time, particularly on an international plane, where Keynesians have argued that there has been a ‘global savings glut’ in trade surplus countries like China, Japan or Germany and their surplus capital has been transferred into the US, driving down interest rates.
…
There is no global or national ‘savings glut’. Instead the problem is an ‘investment dearth’.
…
In my view, low interest rates are not the result of a lack of aggregate demand caused by rising inequality and the inability of workers to buy back their own production. It is the result of the declining profitability of capital in the major capitalist economies
…
Accelerating inflation may be an issue right now in the US and other recovering capitalist economies, and it certainly bites into any recovery in labour incomes; but for capitalism, profitability is the real benchmark and that can be hit by wage rises on the one hand and interest rises on the other. If it is, that is the basis for a new slump.
Pettis: Are We Starting to See Why It’s Really the Exorbitant “Burden”
The role of the U.S. dollar as the world’s global reserve currency has been regarded as a great advantage to the United States but actually it is a destabilizing burden rather than an “exorbitant privilege.”
The Global Housing Market Is Broken, and It’s Dividing Entire Countries
The dream of owning a home is increasingly out of reach. Democratic and authoritarian governments alike are struggling with the consequences.

Other Charts:


Bubble Fare:
China Land Auctions Slump as Developers’ Debt Woes Deepen
Manias, Pandemics, And Crashes
The majority of pundits were claiming last week that the Chinese government would never allow Evergrande to default on its debts. However, this week the company began defaulting on its debts. Now, these same morons are claiming that this Evergrande default is NOT another Lehman event. They claim that this is an isolated event that will have no systemic impacts. They ignore the fact that Evergrande is merely a symptom of a much larger problem.
The problem is moral hazard and the fact that central banks have orchestrated non-stop monetary bailouts since 2008. Now, global speculators no longer fear risk or leverage. They embrace both. Ironically, it's precisely because markets did not sell off this week on news of the default that Beijing has been emboldened to pull the plug on this massive Ponzi scheme.
Quotes of the Week:
Harrison: QE is an asset swap - reserves for Treasuries and MBS. It's not about more money in the system. Like the dot plot, it's about signalling.
Remember, if we weren't at the zero lower bound, the Fed wouldn't be mucking about with these tools. It would cut or raise rates
Harrison: Random thought on the Fed pre-FOMC: The dot plot is not a PREDICTIVE tool. In fact, it is terrible about prediction. It is a SIGNALLING tool. It signals the Fed's present intentions. It doesn't predict the future. That has (limited) value
COVID-19 notes:
More Than Half Of US Companies To Impose Vaccine Mandates, New Survey Finds
Asymptomatic infection is the pandemic’s dark matter
Physicists who study the behavior of galaxies posit the existence of invisible dark matter, which has mass but cannot be seen. The behavior of galaxies cannot be explained without the existence of something we cannot see (1). In this sense, asymptomatic infection is the dark matter of the current severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. Asymptomatic infection is difficult to observe and characterize, by definition, as asymptomatic individuals are not sickened, do not present for care, and cannot be identified without testing. Nonetheless, the frequency with which such infection occurs is key to understanding the epidemiology of the pandemic. In PNAS, Sah et al. (2) provide a rigorous systematic review and metaanalysis of what we know about asymptomatic infection to date. Their review includes 390 studies—a testimonial to the intensity with which this question has been studied. Their results are important: Notwithstanding the virulence of SARS-CoV-2 infection, true asymptomatic infection is common (35%), and asymptomatic infection varies markedly by age, being far less common in older individuals (20%) than in children (47%), with symptomatic infection being more common in long-term care than other settings.
(not just) for the ESG crowd:
Number of Environmental Advocates Killed in 2020 Hits New Record
A recent report found that those killed were most often defending forests against extractive industries.
For the US, the Climate Plan is More Walls and Armed Agents at the Border
China Enforces Power-Rationing At Major Industrial Hubs Amid Shortages And Climate Push

People Vs. Agribusiness Corporations: The Battle Over Global Food and Agriculture Governance
Other Fare:
747-sized asteroid skimmed by Earth, and scientists didn't see it coming
Pics of the Week:
Hubble Has Captured The Startling 'Eye' of a Massive Stellar Explosion
EXTRA [controversial or non-market-related] FARE:
Climate Tweets of the Week:
YOU CANNOT MAKE THIS UP:
Amid floods, wildfires and hurricanes, the Biden administration just issued a ruling declaring that IPCC scientists' new climate report "does not present sufficient cause" to halt a plan for a huge expansion of offshore drilling.
COVID Fare:
The November story
China's account of what happened in Wuhan is incomplete. So too are the accounts of foreign scientists and the American government
OHRC policy statement on COVID-19 vaccine mandates and proof of vaccine certificates.
While receiving a COVID-19 vaccine remains voluntary, the OHRC takes the position that mandating and requiring proof of vaccination to protect people at work or when receiving services is generally permissible under the Human Rights Code (Code) as long as protections are put in place to make sure people who are unable to be vaccinated for Code-related reasons are reasonably accommodated. This applies to all organizations.
Upholding individual human rights while trying to collectively protect the general public has been a challenge throughout the pandemic. Organizations must attempt to balance the rights of people who have not been vaccinated due to a Code-protected ground, such as disability, while ensuring individual and collective rights to health and safety.
…
Receiving a COVID-19 vaccine is voluntary. At the same time, the OHRC’s position is that a person who chooses not to be vaccinated based on personal preference does not have the right to accommodation under the Code.
30 facts you NEED to know: Your Covid Cribsheet
You asked for it, so we made it. A collection of all the arguments you’ll ever need.
You asked for it, so we made it. A collection of all the arguments you’ll ever need.

Fenton: A comparison of age adjusted all-cause mortality rates in England between vaccinated and unvaccinated
In a previous post we argued that the most reliable long-term measure of Covid-19 vaccine effectiveness/safety is the age adjusted all-cause mortality rate. If, over a reasonably prolonged period, fewer vaccinated people die, from whatever cause, including Covid-19, than unvaccinated people then we might conclude that the benefits of the vaccine outweigh the risks. We also pointed out that, to avoid the confounding effect of age, it is critical that data for each age category is available, rather than the aggregated data because, clearly, aggregated data might exaggerate vaccine mortality rates if more older people, with shorter expected mortality, are included.
…The mortality rates for vaccinated against unvaccinated for weeks 1 to 26 of 2021 are charted below. Overall, the chart shows that over time the weighted mortality rate for the vaccinated has steadily increased and by week 16, 23 April 2021, surpassed that for the unvaccinated.
Vanden Bossche: There are many shortcuts to fantasy, but there are no shortcuts to the scientific truth
People asked my opinion about the following article:
“How the unvaccinated threaten the vaccinated for COVID-19: A Darwinian perspective”(Author: Emanuel Goldman)
My comments:
This is yet another example of a professor who thinks he has a good understanding of how this pandemic is evolving and who is firmly convinced he can take advantage of Darwin’s law to put the blame for the catastrophic evolution of this pandemic on the unvaccinated. I am sure he didn’t read my contribution ‘Repetitio est mater studiorum’….
But once, again, let’s get started by assessing his experience in some of the fields that are critically important to understanding the evolutionary dynamics of this pandemic (according to some of the criteria I listed in my contribution ‘Separating the wheat from the chaff’).
Q: Does Goldman understand immunology? No
Q: Does Goldman understand vaccinology? No
So, why does he even try to tackle an issue as complex as a population-level interaction between the host immune system and a virus within the context of mass vaccination?
I’ve inserted my comments below (in italics) in the text of his article. Again, they should illustrate how uninformed, biased interpretations of the data can have a disastrous impact, not only in that they violate the science but also in that they lead to irrational social discrimination. Again, I doubt that Goldman is willing to engage in an open scientific debate on a public platform. He should, therefore, at least seriously consider withdrawing the nonsense he’s trying to sell as a science-based statement.
…
…
As long as the broader public and politicians get advised by incompetent scientists who seem to be addicted to their ego and delusional self-importance, it will be difficult to turn the tide on this pandemic.
Early Treatment vs Stay at Home Until You Can’t Breathe
Why would the CDC aggressively block the compassionate off label use of a “wonder” drug with anti-viral properties taken safely by billions of people around the world for the treatment of parasitic diseases and meriting the Nobel Prize in 2015 for its discoverers? According to Robert F. Kennedy, Jr., the CDC is considered a “captured agency,” a sock puppet for the industry it is supposed to regulate. Half of their budget comes from buying and selling vaccines making it the biggest vaccine distributor in the country.
The mainstream media propaganda campaign has been ramped up to absurd heights of fraud spreading fear-mongering misinformation
… Fraudulent propaganda debunking early treatment has not been limited to the media, but has tainted the most prestigious medical journals in the world.
Ilargi: Crickets
A longtime friend in the US, an emeritus professor, sent me an email recently with a mail exchange between his wife and sister, in which the latter called the Automatic Earth a “conservative website” (first time I heard that one), and said: “When they never cite a source, I call the whole diatribe bullshit. Show me some real, creditable, data, and then we can talk.”
This was in reaction to my September 20 article The Vaccines Kill Many More People Than They Save about Steve Kirsch and his research. I replied -of course- that Kirsch is very meticulous about his sources. And we have more where that came from.
ScienceDirect, an publication by Elsevier, one of the world’s biggest publishers of scientific papers (500,000 a year), has started a special section on Covid named Toxicology Reports: COVID-19 Pandemic: Health impact and Novel research. A recent report in that section is entitled Why Are We Vaccinating Children Against Covid-19?
The authors conclude that there have been at most 35,000 Covid deaths in the US so far, not over 600,000. Because “94 % of the reported deaths had multiple comorbidities”. What could well be over 600,000 is the number of Covid vaccine deaths. Registered VAERS vaccine deaths currently are 14,925.
Basically, they leave nothing standing of the mass vaccination, the vaccine passports, QR codes, none of it. They call the vaccines “treatments” because they don’t comply with the 2000 definition of a vaccine from the U.S. Patent Office, which states “The immune response produced by a vaccine must be more than merely some immune response but must be protective”. They also state that even in the high-risk group of people over 65, the vaccines kill 5 times more people than Covid.
The reason I come back to this -again- is that reports like this, critical of official vaccine policies, and certainly not just in the US, receive no media attention at all. Crickets. It doesn’t even matter who publishes them. You can be the biggest medical publishing house, or the biggest medical journal, the only thing that counts is toeing the party line.
…
Robert W Malone, MD read the report and says: “In summary, the value of these COVID-19 inoculations is not obvious from a cost-benefit perspective for the most vulnerable age demographic, and is not obvious from any perspective for the least vulnerable age demographic.”
“Thus, our extremely conservative estimate for risk-benefit ratio is about 5/1. In plain English, people in the 65+ demographic are five times as likely to die from the inoculation as from COVID-19 under the most favorable assumptions! ” …
There is nothing surprising about the failure of our vaccines. In fact it was totally predictable. Coronavirus vaccines have been used in animals for years, with extremely unimpressive results. The problem is that coronaviruses infect the mucosal surfaces of the lungs, at what is basically the very edge of the reach of our immune systems. You could say that this their grand strategy. They work their way in from our least protected borders. Typically, nasal spray vaccines are preferred in animals to stimulate immunity in the mucosa. Unfortunately, even the sprays achieve immunity that „is often short-lived, requires frequent boosting, and may not prevent re-infection.“ This is after decades of vaccine development and the considerably reduced safety standards observed in veterinary medicine.
Our own SARS-2 vaccines, despite their fancy mRNA and virus vector technology, are entirely of a piece with veterinary standards. They have a poor side effect profile, they provide only temporary and partial protection against infection, and they are deployed on a vast scale with no regard for the evolutionary pressure they place on the virus or their broader consequences for infection dynamics.
Kirsch: Why are the FDA and CDC advisory panel members so afraid to debate COVID Vaccine Safety?
Fast forward to September 17, 2021. I spoke out about the vaccines in the public input section of the FDA advisory meeting. I said that everyone was avoiding the elephant in the room: that the vaccines kill more people than they save. Nobody on the panel was paying attention to my talk. This is pretty typical. I wasn’t offended. But the public was listening and I got millions of impressions on my talk. No one in the mainstream media contacted me to challenge my statement. New results show two stopping conditions were triggered After the meeting, I did some additional research (summarized here) and I discovered that two stopping conditions have been triggered:
• The vaccines have killed over 150,000 Americans. I verified this 7 different ways.
• The vaccines kill more people than they save for all age groups
The most troubling thing to the panel members is that both stopping conditions are now validated in the peer reviewed scientific literature. I have attempted to point this out to the panel in multiple emails which I’ve posted to my Gab account. I offered to share the original research. No interest. I offered to share the studies published in peer-reviewed medical journals backing up what I found. No interest. Next, I offered to donate to their research if they would debate a team of scientists on the two stopping conditions. They could name any donation amount they wanted to make it worth their time. No interest. I pointed out that 100% of the hundreds of people I surveyed wanted to see an open debate on this as soon as possible (and not see the debate happen in slow motion in the scientific literature). No interest. America wants a debate ASAP. The CDC and FDA committee members refuse to discuss this. They won’t debate my team under any conditions.
the vaccinated superspread hypothesis
assessing the riddle of more recovered, more vaccinated, and more dying despite a lower CFR variant
…
high risk cohorts were significantly reduced last year. there is less “dry tinder” now.
we have FAR more people vaccinated now. it’s 50-90% in many places and in many high risk groups. last year it was zero.
and yet in many of the high vaccine uptake places, we’re seeing deaths from covid (and excess mortality) rise to levels ABOVE last year.
this has led many to posit that vaccines not only don’t work, but that they make you worse.
but on an individual level, this does not appear to be true. (though there is quite a lot of evidence that vaccines induce higher risk in the two weeks post administration and that this is being accounted for dishonestly, added to the “unvaccinated” butcher’s bill, and artificially enhancing reported VE.
BUT, even if we control for this, vaccines are showing efficacy in preventing deaths among the vaccinated. it’s more like 50% than the 90%+ being claimed, but VE against death in the 50%’s should still be showing BIG community effects with so many people in the high risk groups vaccinated.
but, on a societal level, it’s not. we’re seeing breakouts to new seasonal highs vs last year and epidemics in covid death rapidly following vaccination campaigns. (MORE)
all else equal even without vaccines, we’d expect to see attenuation in covid deaths for the reasons laid out above. instead we see acceleration.
…
the data has caused a lot of hand wringing and confusion.
grab a seat, because i have an idea to inject into the debate, i sincerely hope that i am wrong, and i suspect a fair few folks are not going to like hearing it, but it’s the best fit i can find for the data.
so here we go: The current surge in covid deaths is caused by the vaccinated. The covid vaccines are extremely leaky and may well accelerate contracting and carrying covid. They allow for very high viral loads to go unnoticed and generate a new and severe asymptomatic spread vector to where none existed before. The high viral loads lead to greater contagion. They may lead to greater severity (but this data is iffy and contested). Vaccine campaigns cause superspread events because vaccination leads to a 2 week window of 40-100% more covid risk that then gets counted as “unvaccinated” because the definitions are bad.
This combination makes those vaccinated with one dose or more into superspread bombs. You get a surge of spread that gets misallocated (and used to inflate ve) and then you get the later breakthrough cases (because the vaccines do not stop infection and just mitigate severity)
These BT cases have massively high VL in often asymptomatic superspreaders that pass on high loading doses to the unvaccinated and greatly worsen the overall pandemic. This further inflates apparent VE by subjecting the unvaccinated to a more profligate and severe disease vector than they would have been had no vaccination campaign ever been undertaken. It moves the whole system to a a different valence. Perversely, if the vaccinated comprise a spread vector that accelerates deaths in the unvaccinated, that would make it look like vaccines work.
Ouch. (told you you weren’t going to like it). In the longer run, this would also select for hotter, deadlier strains because that’s what leaky vaccines do. (more HERE) this would really make life worse for everyone. i want to stress, this is a hypothesis and a work in progress. it’s just the best fit to the facts i can find right now and i REALLY hope it’s wrong because if it’s right, this vaccination campaign is probably the worst health blunder in human history and the epidemiology and politics of that will get stunningly, surreally bad. But if this hypothesis proves out, then calling this an “epidemic of the unvaccinated” is 180 degrees wrong.
It would mean that the unvaxxed are being assaulted by the vaccinated because this vaccine program was incredibly ill conceived and the vaccines are not suited to task and that it, quite literally, was the vaccination programs themselves that have re-intensified what should have been a waning pandemic.
*** The Spartacus Letter (excerpts from first 15 pages of draft, of 41 page PDF, including 26 pages of references with links)
My name is Spartacus, and I’ve had enough.
We have been forced to watch America and the Free World spin into inexorable decline due to a biowarfare attack. We, along with countless others, have been victimized and gaslit by propaganda and psychological warfare operations being conducted by an unelected, unaccountable Elite against the American people and our allies.
Our mental and physical health have suffered immensely over the course of the past year and a half. We have felt the sting of isolation, lockdown, masking, quarantines, and other completely nonsensical acts of healthcare theater that have done absolutely nothing to protect the health or wellbeing of the public from the ongoing COVID-19 pandemic.
Now, we are watching the medical establishment inject literal poison into millions of our fellow Americans without so much as a fight.
We have been told that we will be fired and denied our livelihoods if we refuse to vaccinate. This was the last straw.
We have spent thousands of hours analyzing leaked footage from Wuhan, scientific papers from primary sources, as well as the paper trails left by the medical establishment.
What we have discovered would shock anyone to their core.
First, we will summarize our findings, and then, we will explain them in detail. References will be placed at the end.
Summary:
· COVID-19 is a blood and blood vessel disease. SARS-CoV-2 infects the lining of human blood vessels, causing them to leak into the lungs.
· Current treatment protocols (e.g. invasive ventilation) are actively harmful to patients, accelerating oxidative stress and causing severe VILI (ventilator-induced lung injuries). The continued use of ventilators in the absence of any proven medical benefit constitutes mass murder.
· Existing countermeasures are inadequate to slow the spread of what is an aerosolized and potentially wastewater-borne virus, and constitute a form of medical theater.
· Various non-vaccine interventions have been suppressed by both the media and the medical establishment in favor of vaccines and expensive patented drugs.
· The authorities have denied the usefulness of natural immunity against COVID-19, despite the fact that natural immunity confers protection against all of the virus’s proteins, and not just one.
· Vaccines will do more harm than good. The antigen that these vaccines are based on, SARS-CoV-2 Spike, is a toxic protein. SARS-CoV-2 may have ADE, or antibody-dependent enhancement; current antibodies may not neutralize future strains, but instead help them infect immune cells. Also, vaccinating during a pandemic with a leaky vaccine removes the evolutionary pressure for a virus to become less lethal.
· There is a vast and appalling criminal conspiracy that directly links both Anthony Fauci and Moderna to the Wuhan Institute of Virology.
· COVID-19 vaccine researchers are directly linked to scientists involved in brain-computer interface (“neural lace”) tech, one of whom was indicted for taking grant money from China.
· Independent researchers have discovered mysterious nanoparticles inside the vaccines that are not supposed to be present.
· The entire pandemic is being used as an excuse for a vast political and economic transformation of Western society that will enrich the already rich and turn the rest of us into serfs and untouchables.
COVID-19 Pathophysiology and Treatments:
COVID-19 is not a viral pneumonia. It is a viral vascular endotheliitis and attacks the lining of blood vessels, particularly the small pulmonary alveolar capillaries, leading to endothelial cell activation and sloughing, coagulopathy, sepsis, pulmonary edema, and ARDS-like symptoms. This is a disease of the blood and blood vessels. The circulatory system. Any pneumonia that it causes is secondary to that.
In severe cases, this leads to sepsis, blood clots, and multiple organ failure, including hypoxic and inflammatory damage to various vital organs, such as the brain, heart, liver, pancreas, kidneys, and intestines.
Some of the most common laboratory findings in COVID-19 are elevated D-dimer, elevated prothrombin time, elevated C-reactive protein, neutrophilia, lymphopenia, hypocalcemia, and hyperferritinemia, essentially matching a profile of coagulopathy and immune system hyperactivation/immune cell exhaustion.
COVID-19 can present as almost anything, due to the wide tropism of SARS-CoV-2 for various tissues in the body’s vital organs. While its most common initial presentation is respiratory illness and flu-like symptoms, it can present as brain inflammation, gastrointestinal disease, or even heart attack or pulmonary embolism.
COVID-19 is more severe in those with specific comorbidities, such as obesity, diabetes, and hypertension. This is because these conditions involve endothelial dysfunction, which renders the circulatory system more susceptible to infection and injury by this particular virus.
The vast majority of COVID-19 cases are mild and do not cause significant disease. In known cases, there is something known as the 80/20 rule, where 80% of cases are mild and 20% are severe or critical. However, this ratio is only correct for known cases, not all infections. The number of actual infections is much, much higher. Consequently, the mortality and morbidity rate is lower. However, COVID-19 spreads very quickly, meaning that there are a significant number of severely-ill and critically-ill patients appearing in a short time frame.
In those who have critical COVID-19-induced sepsis, hypoxia, coagulopathy, and ARDS, the most common treatments are intubation, injected corticosteroids, and blood thinners. This is not the correct treatment for COVID-19. In severe hypoxia, cellular metabolic shifts cause ATP to break down into hypoxanthine, which, upon the reintroduction of oxygen, causes xanthine oxidase to produce tons of highly damaging radicals that attack tissue. This is called ischemia-reperfusion injury, and it’s why the majority of people who go on a ventilator are dying. In the mitochondria, succinate buildup due to sepsis does the same exact thing; when oxygen is reintroduced, it makes superoxide radicals. Make no mistake, intubation will kill people who have COVID-19.
The end-stage of COVID-19 is severe lipid peroxidation, where fats in the body start to “rust” due to damage by oxidative stress. This drives autoimmunity. Oxidized lipids appear as foreign objects to the immune system, which recognizes and forms antibodies against OSEs, or oxidation-specific epitopes. Also, oxidized lipids feed directly into pattern recognition receptors, triggering even more inflammation and summoning even more cells of the innate immune system that release even more destructive enzymes. This is similar to the pathophysiology of Lupus.
COVID-19’s pathology is dominated by extreme oxidative stress and neutrophil respiratory burst, to the point where hemoglobin becomes incapable of carrying oxygen due to heme iron being stripped out of heme by hypochlorous acid. No amount of supplemental oxygen can oxygenate blood that chemically refuses to bind O2.
The breakdown of the pathology is as follows:
….
…
The correct treatment for severe COVID-19 related sepsis is non-invasive ventilation, steroids, and antioxidant infusions. Most of the drugs repurposed for COVID-19 that show any benefit whatsoever in rescuing critically-ill COVID-19 patients are antioxidants. N-acetylcysteine, melatonin, fluvoxamine, budesonide, famotidine, cimetidine, and ranitidine are all antioxidants. Indomethacin prevents iron-driven oxidation of arachidonic acid to isoprostanes. There are powerful antioxidants such as apocynin that have not even been tested on COVID-19 patients yet which could defang neutrophils, prevent lipid peroxidation, restore endothelial health, and restore oxygenation to the tissues.
…
Scientists who know anything about pulmonary neutrophilia, ARDS, and redox biology have known or surmised much of this since March 2020. In April 2020, Swiss scientists confirmed that COVID-19 was a vascular endotheliitis. By late 2020, experts had already concluded that COVID-19 causes a form of viral sepsis. They also know that sepsis can be effectively treated with antioxidants. None of this information is particularly new, and yet, for the most part, it has not been acted upon. Doctors continue to use damaging intubation techniques with high PEEP settings despite high lung compliance and poor oxygenation, killing an untold number of critically ill patients with medical malpractice.
Because of the way they are constructed, Randomized Control Trials will never show any benefit for any antiviral against COVID-19. Not Remdesivir, not Kaletra, not HCQ, and not Ivermectin. The reason for this is simple; for the patients that they have recruited for these studies, such as Oxford’s ludicrous RECOVERY study, the intervention is too late to have any positive effect.
…
In these trials, they give antivirals to severely ill patients who have no virus in their bodies, only a delayed hyperinflammatory response, and then absurdly claim that antivirals have no utility in treating or preventing COVID-19. These clinical trials do not recruit people who are pre-symptomatic. They do not test pre-exposure or post-exposure prophylaxis.
This is like using a defibrillator to shock only flatline, and then absurdly claiming that defibrillators have no medical utility whatsoever when the patients refuse to rise from the dead. The intervention is too late. These trials for antivirals show systematic, egregious selection bias. They are providing a treatment that is futile to the specific cohort they are enrolling.
India went against the instructions of the WHO and mandated the prophylactic usage of Ivermectin. They have almost completely eradicated COVID-19. The Indian Bar Association of Mumbai has brought criminal charges against WHO Chief Scientist Dr. Soumya Swaminathan for recommending against the use of Ivermectin.
Ivermectin is not “horse dewormer”. Yes, it is sold in veterinary paste form as a dewormer for animals. It has also been available in pill form for humans for decades, as an antiparasitic drug.
The media have disingenuously claimed that because Ivermectin is an antiparasitic drug, it has no utility as an antivirus. This is incorrect. Ivermectin has utility as an antiviral. It blocks importin, preventing nuclear import, effectively inhibiting viral access to cell nuclei. Many drugs currently on the market have multiple modes of action. Ivermectin is one such drug. It is both antiparasitic and antiviral.
In Bangladesh, Ivermectin costs $1.80 for an entire 5-day course. Remdesivir, which is toxic to the liver, costs $3,120 for a 5-day course of the drug. Billions of dollars of utterly useless Remdesivir were sold to our governments on the taxpayer’s dime, and it ended up being totally useless for treating hyperinflammatory COVID-19. The media has hardly even covered this at all.
The opposition to the use of generic Ivermectin is not based in science. It is purely financially and politically-motivated. An effective non-vaccine intervention would jeopardize the rushed FDA approval of patented vaccines and medicines for which the pharmaceutical industry stands to rake in billions upon billions of dollars in sales on an ongoing basis.
…
COVID-19 is airborne. …. Surgical masks do not protect you from aerosols. The virus is too small and the filter media has too large of gaps to filter it out. They may catch respiratory droplets and keep the virus from being expelled by someone who is sick, but they do not filter a cloud of infectious aerosols if someone were to walk into said cloud.
The minimum level of protection against this virus is quite literally a P100 respirator, a PAPR/CAPR, or a 40mm NATO CBRN respirator, ideally paired with a full-body tyvek or tychem suit, gloves, and booties, with all the holes and gaps taped.
…
The vaccines for COVID-19 are not sterilizing and do not prevent infection or transmission. They are “leaky” vaccines. This means they remove the evolutionary pressure on the virus to become less lethal. It also means that the vaccinated are perfect carriers. In other words, those who are vaccinated are a threat to the unvaccinated, not the other way around.
All of the COVID-19 vaccines currently in use have undergone minimal testing, with highly accelerated clinical trials. Though they appear to limit severe illness, the long-term safety profile of these vaccines remains unknown.
Some of these so-called “vaccines” utilize an untested new technology that has never been used in vaccines before. Traditional vaccines use weakened or killed virus to stimulate an immune response. The Moderna and Pfizer-BioNTech vaccines do not. They are purported to consist of an intramuscular shot containing a suspension of lipid nanoparticles filled with messenger RNA. The way they generate an immune response is by fusing with cells in a vaccine recipient’s shoulder, undergoing endocytosis, releasing their mRNA cargo into those cells, and then utilizing the ribosomes in those cells to synthesize modified SARS-CoV-2 Spike proteins in-situ.
These modified Spike proteins then migrate to the surface of the cell, where they are anchored in place by a transmembrane domain. The adaptive immune system detects the non-human viral protein being expressed by these cells, and then forms antibodies against that protein. This is purported to confer protection against the virus, by training the adaptive immune system to recognize and produce antibodies against the Spike on the actual virus. The J&J and AstraZeneca vaccines do something similar, but use an adenovirus vector for genetic material delivery instead of a lipid nanoparticle. These vaccines were produced or validated with the aid of fetal cell lines HEK-293 and PER.C6, which people with certain religious convictions may object strongly to.
SARS-CoV-2 Spike is a highly pathogenic protein on its own. It is impossible to overstate the danger presented by introducing this protein into the human body.
It is claimed by vaccine manufacturers that the vaccine remains in cells in the shoulder, and that SARS-CoV-2 Spike produced and expressed by these cells from the vaccine’s genetic material is harmless and inert, thanks to the insertion of prolines in the Spike sequence to stabilize it in the prefusion conformation, preventing the Spike from becoming active and fusing with other cells. However, a pharmacokinetic study from Japan showed that the lipid nanoparticles and mRNA from the Pfizer vaccine did not stay in the shoulder, and in fact bioaccumulated in many different organs, including the reproductive organs and adrenal glands, meaning that modified Spike is being expressed quite literally all over the place. These lipid nanoparticles may trigger anaphylaxis in an unlucky few, but far more concerning is the unregulated expression of Spike in various somatic cell lines far from the injection site and the unknown consequences of that.
…
SARS-CoV-2 Spike has a Superantigenic region (SAg), which may promote extreme inflammation.
Anti-Spike antibodies were found in one study to function as autoantibodies and attack the body’s own cells. Those who have been immunized with COVID-19 vaccines have developed blood clots, myocarditis, Guillain-Barre Syndrome, Bell’s Palsy, and multiple sclerosis flares, indicating that the vaccine promotes autoimmune reactions against healthy tissue.
…
SARS-CoV-2 Spike has a prion-like domain that enhances its infectiousness.
The Spike S1 RBD may bind to heparin-binding proteins and promote amyloid aggregation. In humans, this could lead to Parkinson’s, Lewy Body Dementia, premature Alzheimer’s, or various other neurodegenerative diseases. This is very concerning because SARS-CoV-2 S1 is capable of injuring and penetrating the blood-brain barrier and entering the brain. It is also capable of increasing the permeability of the blood-brain barrier to other molecules.
SARS-CoV-2, like other betacoronaviruses, may have Dengue-like ADE, or antibody-dependent enhancement of disease. For those who aren’t aware, some viruses, including betacoronaviruses, have a feature called ADE. There is also something called Original Antigenic Sin, which is the observation that the body prefers to produce antibodies based on previously-encountered strains of a virus over newly-encountered ones.
In ADE, antibodies from a previous infection become non-neutralizing due to mutations in the virus’s proteins. These non-neutralizing antibodies then act as trojan horses, allowing live, active virus to be pulled into macrophages through their Fc receptor pathways, allowing the virus to infect immune cells that it would not have been able to infect before. This has been known to happen with Dengue Fever; when someone gets sick with Dengue, recovers, and then contracts a different strain, they can get very, very ill.
If someone is vaccinated with mRNA based on the Spike from the initial Wuhan strain of SARS-CoV-2, and then they become infected with a future, mutated strain of the virus, they may become severely ill. In other words, it is possible for vaccines to sensitize someone to disease.
…
We have been told that SARS-CoV-2 mRNA vaccines cannot be integrated into the human genome, because messenger RNA cannot be turned back into DNA. This is false. … it is possible that people who take this vaccine may continuously express SARS-CoV-2 Spike from their somatic cells for the rest of their lives.
By inoculating people with a vaccine that causes their bodies to produce Spike in-situ, they are being inoculated with a pathogenic protein. A toxin that may cause long-term inflammation, heart problems, and a raised risk of cancers. In the long-term, it may also potentially lead to premature neurodegenerative disease.
Absolutely nobody should be compelled to take this vaccine under any circumstances, and in actual fact, the vaccination campaign must be stopped immediately.
COVID-19 Criminal Conspiracy:
The vaccine and the virus were made by the same people.
…
In November of 2019, three technicians at the Wuhan Institute of Virology developed symptoms consistent with a flu-like illness. Anthony Fauci, Peter Daszak, and Ralph Baric knew at once what had happened, because back channels exist between this laboratory and our scientists and officials.
December 12th, 2019, Ralph Baric signed a Material Transfer Agreement (essentially, an NDA) to receive Coronavirus mRNA vaccine-related materials co-owned by Moderna and NIH. It wasn’t until a whole month later, on January 11th, 2020, that China allegedly sent us the sequence to what would become known as SARS-CoV-2. Moderna claims, rather absurdly, that they developed a working vaccine from this sequence in under 48 hours.
…
The animal reservoir of SARS-CoV-2 has never been found.
This is not a conspiracy “theory”. It is an actual criminal conspiracy, in which people connected to the development of Moderna’s mRNA-1273 are directly connected to the Wuhan Institute of Virology and their gain-of-function research by very few degrees of separation, if any. The paper trail is well-established.
The lab-leak theory has been suppressed because pulling that thread leads one to inevitably conclude that there is enough circumstantial evidence to link Moderna, the NIH, the WIV, and both the vaccine and the virus’s creation together. In a sane country, this would have immediately led to the world’s biggest RICO and mass murder case. Anthony Fauci, Peter Daszak, Ralph Baric, Shi Zhengli, and Stéphane Bancel, and their accomplices, would have been indicted and prosecuted to the fullest extent of the law. Instead, billions of our tax dollars were awarded to the perpetrators.
…
The establishment is cooperating with, and facilitating, the worst criminals in human history, and are actively suppressing non-vaccine treatments and therapies in order to compel us to inject these criminals’ products into our bodies.
…
COVID-19 Vaccine Development and Links to Transhumanism:
This section deals with some more speculative aspects of the pandemic and the medical and scientific establishment’s reaction to it, as well as the disturbing links between scientists involved in vaccine research and scientists whose work involved merging nanotechnology with living cells.
…
Since these revelations, it has come to the attention of independent researchers that the COVID-19 vaccines may contain reduced graphene oxide nanoparticles. Japanese researchers have also found unexplained contaminants in COVID-19 vaccines.
…
Conclusions:
The current pandemic was produced and perpetuated by the establishment, through the use of a virus engineered in a PLA-connected Chinese biowarfare laboratory, with the aid of American taxpayer dollars and French expertise.
This research was conducted under the absolutely ridiculous euphemism of “gain-of-function” research, which is supposedly carried out in order to determine which viruses have the highest potential for zoonotic spillover and preemptively vaccinate or guard against them.
Gain-of-function/gain-of-threat research, a.k.a. “Dual-Use Research of Concern”, or DURC, is bioweapon research by another, friendlier-sounding name, simply to avoid the taboo of calling it what it actually is. It has always been bioweapon research. The people who are conducting this research fully understand that they are taking wild pathogens that are not infectious in humans and making them more infectious, often taking grants from military think tanks encouraging them to do so.
These virologists conducting this type of research are enemies of their fellow man, like pyromaniac firefighters. GOF research has never protected anyone from any pandemic. In fact, it has now started one, meaning its utility for preventing pandemics is actually negative. It should have been banned globally, and the lunatics performing it should have been put in straitjackets long ago.
Either through a leak or an intentional release from the Wuhan Institute of Virology, a deadly SARS strain is now endemic across the globe, after the WHO and CDC and public officials first downplayed the risks, and then intentionally incited a panic and lockdowns that jeopardized people’s health and their livelihoods.
This was then used by the utterly depraved and psychopathic aristocratic class who rule over us as an excuse to coerce people into accepting an injected poison .. They believe they can get away with this by weaponizing the social stigma of vaccine refusal. They are incorrect.
…
Why are they doing this? Simple. The Elites are Neo-Malthusians and believe that we are overpopulated and that resource depletion will collapse civilization in a matter of a few short decades. They are not necessarily incorrect in this belief. We are overpopulated, and we are consuming too many resources. However, orchestrating such a gruesome and murderous power grab in response to a looming crisis demonstrates that they have nothing but the utmost contempt for their fellow man.
Freedom prevails: COVID data shows ‘public health’ mandates only harm people
There’s something about human nature that causes people in power to want to “do something” when faced with an unknown problem. Yet sometimes, doing nothing is better than “doing something.” When it comes to the COVID-19 pandemic, more and more evidence is emerging that the laissez-faire approach to the issue — at least on a governmental/”public health” level — was the solution all along. The path chosen by Sweden, Belarus and a select few nations — which put the power in the hands of individuals to make their own health choices, instead of imposing draconian government edicts — appears to have won the day. With almost two years of data now in our hands, it sure seems that the ruling class has a lot to answer for.
Since the first COVID-19 outbreak in Wuhan, China, in early 2020, the supposed expert class has told us that their forcible “mitigation and suppression” tools, such as lockdowns, masks, and social distancing via government edicts, were absolutely necessary to prevent incredible potential damage that would have been caused by the apparent unchecked circulation of this virus. The “experts” overwhelmingly endorsed these Chinese Communist Party-endorsed “health” measures, declaring them scientific overnight, despite many of these tools never being utilized in the event of a global pandemic. Far from looking back to reassess the premise of their grand plans, these leaders continued to plow forward with further and further restrictions on our liberties. They then pivoted to using these instruments of power in combination with compulsory therapy regimes, all under the guise of keeping us simple-minded plebs safe from the virus. Sure, all of our unalienable rights were seemingly stripped away without due process, but governments assured us that these supposedly scientifically proven measures would shield us from COVID-19. At the very least, we were told that these restrictions would be worth it because they are “keeping us safe.”
Now, almost two years have passed, and there is simply no evidence to date that these measures helped with our virus problem. In fact, given the excess death data of laissez-faire Sweden, you can now make the case that these “public health” solutions actually caused far more health problems than COVID-19 ever could by itself.
Excess deaths data tell us an incredible tale. Sweden has been largely open and free from any restrictions for 15 months and counting, and Stockholm has seen virtually *zero* excess deaths from the “deadly pandemic.”
*** Denninger: Once Upon A Time…
… in a not-so-tiny nation called Spain, a nursing home had a nasty virus get into it. It was March of 2020. The nasty virus was called Covid-19. And this nursing home, like so many others all over the world, was full of elderly, morbid people. The mean age of residents was 85 and 48% were over 80 years old. It was a killing field, like so many others….. Within three months 100% of the residents had caught the virus. Not presumed to have — proved to have. How do we know this? Because almost every one of them seroconverted. All but three out of 84 of them, to be precise. Think about that last sentence for a second. Almost every one of them seroconverted. How’s that possible? Many of them died, right? You can’t seroconvert if you’re dead.
No. Not only did nearly none die none went to the hospital either because they rapidly figured out how to stop the virus from killing people — and did exactly that. You would have thought this would have been all over the news. In point of fact not one mention of it was made. Further, not one write-up was made in medical journals either until January of 2021, which I missed. My bad — out of the several hundred medical journal pieces, I missed this one. It was brought to my attention on my forum and my jaw immediately hit the floor. The jab train must continue, you see. So must the ventilator train. So must the money train, the mask train and the rest of the BS we have endured for the last 18+ months. So must the slaughter for money, the fear, and the lies. So what did these few nursing homes do that nobody has done since and nobody reported out at the time?
1. Early start of treatment, regardless of the severity of patient symptoms.
– Antihistamines every 12 h: dexchlorpheniramine 2 mg, cetirizine 10 mg or loratadine 10 mg.
– Azithromycin 500 mg orally every 24 h for 3 days if there is rapid improvement, and for 6 days if the duration of symptoms is prolonged.
– If pain or fever, acetaminophen 650 mg/6–8 h.
– Nasal washing and gargling with sodium bicarbonate water (half a glass of warm water with half a teaspoon of sodium bicarbonate).
2. Patients with mild or recent-onset symptoms (cough, fever, general malaise, anosmia, polymyalgia):
– Antihistamines + Azithromycin (see mild treatment management)
– Levofloxacin 500 mg/12 h, up to 14 days of antibiotic treatment from diagnosis.
– Mepifilin solution, 50 mg/8 h as a bronchodilator, until subjective improvement. Patients with previous lung disease (asthma or COPD) used their usual bronchodilators.
– If the patient experienced increased breathing difficulty, prednisone 1 mg/kg/day divided into two doses until clinical improvement, and then it was slowly tapered down.
3. If symptoms of severity (dyspnea, breathing difficulty, mild or moderate chest pain, with SpO2 >80%, heart rate <100 beats per minute at any time of the process):
4. Prophylactic treatment for close contacts, including all asymptomatic residents:
– Antihistamines at the same dose as symptomatic patients.
Look at that top line.
Cetrizine is otherwise known as Zyrtec. Loratadine is otherwise known as Claritin. Dexchlorpheniramine is not often-used in the US anymore, but it used to be. The other two core drugs were Azithromycin and Levofloxacin, both common antibiotics with the first being the infamous "Zpak" from the HCQ+Zinc+Zpak combination that a fraudulent study was used to discredit.
Both of the first two antihistamines are available over the counter in most nations including the United States. The dosing they used is twice that on the label. The two antibiotics are both available anywhere for little money.
Before they started treating people three residents died. The entire group of them had the common maladies of old age -- hypertension, diabetes, COPD, cardiovascular disease. Most were using a huge range of existing drugs for their conditions (5 or more.)
As soon as they started treating people the following happened:
All of our patients evolved satisfactorily and were recovered at the beginning of June. No adverse effects were recorded in any patient and no one required hospital admission. At the end of June, 100% of the residents and almost half of the workers had positive serology for COVID-19, most of them with past infection.
Not one adverse event occurred among these residents and staff and no hospitalizations were necessary either.
In pooled data 28% of the residents in similar nursing homes over the same time period died. In these two, once they started treating with cheap drugs, leading with those available over the counter in the US, ZERO -- I repeat -- ZERO had a bad reaction to the protocol, ZERO died and ZERO were admitted to a hospital for treatment.
ZERO.
It was one hundred percent effective.
Yes, it's a small sample. Go do the statistical math on the CI for that size sample and results if you insist.
According to the mechanisms of action described, these drugs would act synergistically in the early stages of the disease, which is why we consider it essential to start the treatment as soon as possible. Once the virus has colonized the respiratory system, the effectiveness is probably more limited, and hence the failure of these treatments in more advanced stages of the disease, when hospital admission is necessary. In our experience, early double antibiotics were effective to control the process in cases with moderate symptoms.
Nobody cared.
Nobody reported on this.
Nobody duplicated it either.
I didn't even realize this study existed; had I known of it guess what I would have added to my protocol when I got Covid-19 the first week of August of this year, since it happens to be in my medicine cabinet already for seasonal allergies? Uh huh. Two 60ct bottles of generic Claritin equivalent costs about $12 at WalMart.
Folks, think about this long and hard: In the worst-case scenario for those who this virus should have killed -- it killed nobody. It should be killing statistically nobody today -- right here, right now. How to prevent it from doing so was discovered in March and April of 2020 and intentionally ignored worldwide.
It is still being ignored today.
With these numbers there is no reason to fear a Covid-19 infection. There is no reason to take a vaccine. There was never a reason to develop a vaccine, especially the ones we have today; infection that does not produce severe disease is sterilizing and thus wildly superior to vaccinated immunity which is now proved to be failing worldwide. There is no reason to wear a mask.
Every single one of these residents seroconverted and became immune with mild or moderate symptoms consistent with seasonal colds and flus and not one of them was put into the hospital or killed. The treatment is so ******ned cheap and available there's no excuse to not use it instantly on suspicion of infection and prophylactically among everyone else in your household at first sign of trouble.
You think the entire load of BS around HCQ and Ivermectin is bad? This is a thousand times worse.
Those who died did not do so due to a "novel coronavirus"; we knew how to treat that infection successfully for pennies in March and April of 2020. Yes, in the first month or two people died because we did not know.
Beyond April of 2020 people died because we let the medical system and governments murder them for profit and they're still doing it today. We, the people, have allowed this. We have failed and refused to rise up and hold accountable, personally, every single hospital, doctor, so-called "hero" nurse and every single politician across the globe. They willfully and intentionally slaughtered millions on a global basis.
The answer to the problem -- to Covid-19 -- was known in March and April of 2020 and yet not published until January of this year, and even then not one single bit of media attention nor a single mention from Fauci, the CDC, the NIH or FDA has been made, all in the interest of Moderna and Pfizer's stock prices and the power-mad jackasses on an international basis -- at the cost of your loved ones' lives.
That wasn't an accident and it still isn't one.
Mathew Crawford: Confirmation of Vaccine-Associated Mortality
Okay, okay, let's take a look at what Kostoff et al found:
A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreases drastically as age decreases, and the longer-term effects of the inoculations on lower age groups will increase their risk-benefit ratio, perhaps substantially.Apologies to anyone who just fell out of their chair and bumped their asshole. Read it again if you need to.
Kostoff also departs from the narrative by expressing concern over life-changing harms to young people given the much longer life expectancies and quality years they have in front of them.
For example, the trials and VAERS reported clots that resulted in serious symptoms and deaths but gave no indication of the enhanced predisposition to forming serious clots in the future with a higher base of micro-clots formed because of the mRNA intervention. The latter is particularly relevant to children, who have a long future that could be seriously affected by having an increased predisposition to multiple clot-based (and other) serious diseases resulting from these inoculations.Sometimes, I read a paragraph, reflect on authors with competing opinions, and ask myself, "Who do I want to trust (on a human level)?" Such a bias does not get to definite answers, of course, but I strongly suspect there is a high correlation.
Note for those who want to read this paper for full understanding: While you can understand the analysis in many papers on a fundamental level without reading the appendices, this paper is not one of those. Nearly the full meat of the analyses are in the appendices, which is to say that the primary text serves somewhat like an abstract. And for those worried about the background deaths rate computations, Kostoff and crew provide a short-range sensitivity analysis.
In light of these data, the question may arise as to why there were no inoculant-attributed deaths in clinical testing of inoculants. The answer is that neither Pfizer nor Moderna included frail patients and included only a small number of very elderly patients - those over 75 accounted for 4.4 % of the total tested for Pfizer and 4.1 % for Moderna. While they could not in fact determine a causal relationship between inoculation and death, they also could not rule out that the inoculations had accelerated the deterioration of the condition of those patients [33].Right here. Kostoff and his team state what should be obvious to anyone who cares about an honest assessment---that there is a need to examine bodies to ascertain anything like a positive risk-benefit assessment of the vaccines. This is true both on the level of autopsies, but also on the level of seriously harmed patients whose life expectancies and quality years may now be significantly reduced. Maybe this is the moment to point out that no human even uttered the phrase "mild cases of myocarditis" prior to the CDC's recognition of the avalanche of such cases in young recipients of COVID-19 vaccines. Such heart damage is permanent, often results in dramatically shortened life spans, and can result in unpredictable sudden death at any time.
That is to say that when either Steve Kirsch or I claim there may be 150,000 to 250,000 deaths associated with COVID-19 vaccines, we may be talking about a floor. The true number will likely expand---maybe dramatically---over the coming years. This is a truly large-scale and still ongoing human tragedy.
And while the risk-benefit analysis doesn't look good for anyone taking the vaccines, it looks absurd and frightening for children. Emphasis mine.
What does this mean in the real world? In the USA, there are approximately 4,000,000 children in each age year for adolescents. Thus, there are ˜16,000,000 children in the 12–15 age band. A serious adverse event, including death, that occurred at a 1/800 rate would not be detectable with high confidence in a sample of 1005 people. Thus, the results of the trials for 1005 children would allow for 20,000 children to suffer a non-trial-detected serious adverse event, including death, when extrapolated to potential inoculation of all children in the 12–15 age group! Given that the risk of contracting COVID-19 with serious outcomes is negligible in this population, proceeding with mass inoculation of children 12–15 years old based on the trials that were conducted cannot be justified on any cost-benefit ratio findings.
Medical Cruelty and Loving Attention
Earlier tonight, somebody sent me this page at Medscape. It's revealing. Let's take a look at a sample of what doctors around the world are saying about the COVID-19 vaccines.
…
It goes on and on and on.
…
I feel deeply for these doctors. They're fighting wars on several fronts, and must sometimes take gaslighting from their own peers.
COVID-19 Research Pop Quiz (And Then Some?)
Much of the reason that a pandemic could be stretched to "max pain" is that the firehose of information achieves the effect of miseducating the public. Even worse, those in charge of the firehose point the finger at people like me and tell the public that we're the disinformation warriors. I've been banned from Facebook for roughly 100 of the past 300 days for crimes that range from sharing information from a meeting I joined in with an Indian Council of Medical Research physician, to showing a packet of ivermectin (out of India), and to stating that it's okay for parents to defend their children with force.
… So, what, if anything, could short-circuit such diabolical propaganda machinery? How can the public get a glimpse of all the absurdity? How do you educate people who cannot fathom that they've been miseducated? Fighting them over social media all day ain't gonna do squat [except in true edge cases]. We need solutions to challenging social problems that take into account the realities of brainwashing, groupthink, proxy-trust, social pressure, and maybe also gamification principles.
CO-VID of the Week:
More Evidence That They Know the Covid Vaccine Is Killing and Maiming People and Yet They Continue Their Death Program
Here is a doctor and chief RN in a US Department of Health & Human Services Hospital reporting that the official protocol is NOT to report adverse reactions to the vaccine, NOT to treat Covid patients with safe and effective Ivermectin, indeed, it is impermissible to do so and you are fired if you save lives with Ivermectin, and NOT to permit staff to refuse inoculation based on informed consent from seeing the deadly effects of the vaccine on patients.
In this video you can witness the doctor and nurses speaking about the evil of the Health & Human Services federal hospital intentionally killing people and preventing doctors and nurses from saving the lives of patients. This is not happening from incompetence and lack of knowledge. People are being systematically murdered, and Covid is being blamed. All adverse vaccine reactions are blamed on Covid, not on the vaccine, and this lie is used to justify not reporting the adverse event.
You had better watch the brief video before it is taken down as “Covid disinformation.” It is a video of doctors and nurses on the front line discussing what they see and experience
COVID Quotes of the Week:
In an alternate universe the governments of a parallel Earth responded to the pandemic by pouring money into healthcare systems, transferring wealth from their nations’ richest to their poorest, and saying “Here’s a new vaccine but it’s up to you whether you use it or not.”
Gatito Bueno: i am just a kitten and not an epidemiological tracking expert, but do you guys think that maybe when the CDC starts to disavow the VAERS system that it’s probably not sign that things are going super well?
parents opting out for ‘philosophical reasons’ are mostly white and mostly wealthy…. Parents who opt out of vaccines tend to “believe, simply, that they can make the scientific determinations about the efficacy and dangers of vaccines for themselves,”
Mathew Crawford: A new hero has emerged. Mostly-retired scientist Ronald Kostoff, PhD, and a highly experienced team, just had their paper published. The appropriate, if understated title of the paper is: Why are we vaccinating children against COVID-19? Let us appreciate his restraint in never using the word "assholes" anywhere in the paper. At the age of 84, he maintains a level of polite discipline in the face of assholes I can scarcely muster on my better days.
COVID Tweets of the Week:
Highly effective home care kits in India & Latin America avg cost $2.65 shows why this hasn’t happened in “developed” world.
Avg vaxx cost $16.25/dose Pfizer, $19.20 Moderna x2 +boosters. Manufacturing cost $2.85/dose.
Recovery w/home care likely immune 4 life w/o side effects.
Kulldorff: By mandating vaccines for those who have had COVID, @NIAIDNews director Anthony Fauci questions natural immunity after COVID disease. That's like having the nation’s lead astronomer question whether the earth is round or flat.
Kory: Uttar Pradesh COVID cases now effectively ZERO given population of 241 million, massive testing, 5% vax. Rivals the historic eradications of smallpox & polio with vaccines, except those were celebrated in all the papers and all the streets… while UP’s IVM strategy.. not a peep
Did they force people who already had Covid to get the vaccine in order to inflate the success rate of the vaccine by embedding natural immunity into the data?
Yes, forcing people out of their jobs and into poverty because of a personal medical decision is wrong, actually.
On the eve of the introduction of medical apartheid in Ontario what may be hardest to deal with is that the large majority —your friends, family, colleagues, strangers—*support* government banning you and so many others from society.
Forgive them, for they know not what they do.
COVID Conspiracy Fare:
10+ Years to Stop the Spread
We’re not getting out of this pandemic anytime soon. The government has no idea what they’re doing, they manipulate the numbers of cases and deaths, they lie to us constantly, they’re rationing therapeutics and they’ve allowed more than a million illegal aliens into the country this year during a pandemic. It’s obvious that the democrats don’t want COVID-19 going anywhere. And who can blame them? It helped them get rid of Trump by cheating in an election and has allowed them to be able to rule over us tyrannically in every facet of government – federal, state, county, city, townships, health departments, school boards, OSHA, licensing boards and more.
Everyone and their brother (and sister) in government has been trying to control what we do and take away our freedoms – presidents, governors, mayors, attorney generals, health directors, and local commissioners. The democrats have also been able to control us with school boards, leftist businesses, social media and the fake news on their side. COVID-19 was a gift to the democrats and it’s a gift that keeps on giving. They have no intention to let it go. At this point, it really doesn’t matter how many vaccines and therapeutics we come up with because we can’t end a pandemic with open borders and a democrat president who ships these people all over the country. So we’re going to have to learn to live with the pandemic for a long long time – and different variants of the virus.
Because of this, I have a kind of apocalyptic prediction that this will end up being an extinction level event. I’m not sure what the timeline is. Five years, ten years, maybe more if we slow it down a bit here and there. But I’m starting to believe that the virus will stop spreading when a large percentage of the people on the planet stop breathing. There are too many leftists around the world keeping this thing going. But the democrats will be okay with that because it means a lot less carbon dioxide being emitted into the air from that breathing. A lot less cows will needed for food, a lot less cars will be driving around and a lot less airplanes will be flying in the skies. So it’s pretty much a winning situation if the virus goes on for a while and destroys a lot of people in its path. The only way the democrats DON’T win is if the virus is beaten. And the democrats NEVER want to lose. Think about that.
GeoPolitical Fare:
Whitney Webb: The Politics of Fear and Self-Preservation
Many of those who have been quick and vocal to point out the lies of the US government when it comes to the invasions of Afghanistan and Iraq and other consequences of the War on Terror have been unable to even consider that the official story of 9/11 may not be legitimate and may indeed have been dealt from the same pack. This may be for a variety of reasons, including a strong desire to not be de-legitimized by their peers as bearers of the “conspiracy theorist” smear and an unwillingness to face a political reality where US government officials may have been complicit in a deadly attack on American soil. In those two examples, however, the failure of such individuals, particularly in media, to even consider that there may be more to the story boils down to a desire for self-preservation in the case of the former and preservation of a particular worldview in the case of the latter.
Yet, in both cases, the casualty is the truth and the cause is cowardice. By failing as a society to thoroughly examine the events of 9/11 and why those events occurred, the American public has shown the powers that be that their desire to preserve a “safe” worldview — and to preserve their own careers, in the case of certain professional classes — is enough to keep people from questioning world-altering events when they emerge. Those powers are well aware of this refusal and have been using it to their advantage ever since. Today, with the COVID-19 crisis still dragging on, we are similarly immersed in a situation where nuance and facts are being cast aside, militantly in some cases, in favor of the establishment narrative. Is everyone who chooses not to take this particular vaccine a “conspiracy theorist” and “anti-vaxxer”?
Does it really make sense to so dramatically divide the public into groups of vaccinated and unvaccinated through a new ID system when the vaccine claims to reduce the severity of illness but not to stop disease transmission? Should those that question the motivation of politicians, powerful pharmaceutical corporations and mainstream media “experts” be censored from expressing those views online? You do not need to agree with those who hold such views, but what is wrong with hearing what they have to say and debating their evidence with your own?
We are losing the ability to have rational public discourse about these issues — and losing it swiftly, at a speed comparable to what took place in the aftermath of 9/11, when questioning the motives of the Bush administration, US intelligence agencies and other groups, as well as their proposed responses and “solutions,” was deemed “unpatriotic” and even “treasonous” by some. Calls were made to strip an entire class of Americans of their freedom for merely sharing the same ethno-religious identities as those we were told attacked us, and many went along with it. Freedom became treated as a privilege only for certain groups, not as a right, and this insidious fallacy has reared its head yet again in recent months in relation to the COVID-19 vaccine debate and also the war on domestic terror.
Greenwald: New Proof Emerges of the Biden Family Emails: a Definitive Account of the CIA/Media/BigTech Fraud
An axis of the CIA, Big Tech and the DNC-allied wing of the corporate media spread an absolute lie in the weeks before the 2020 election. We now have definitive proof.
The Horses' Asses of the Apocalypse
The worst thing about the atrocious treatment of the Haitian refugees for Biden, though, is that the photographic evidence of systemic US cruelty - rather than the cruelty itself - is an embarrassment to him personally. It makes him look bad, especially when the images were released just as he was belligerently touting American peace, love, democracy and freedom to the rest of the world at the United Nations' annual summit this week.
“It’s an embarrassment. It’s beyond an embarrassment. It’s dangerous, it’s wrong, it sends the wrong message around the world or sends the wrong message at home," he fumed, ending his spiel with the obligatory "It's not who we are!"
It's hard emphasize enough just how craven and downright psychopathic this statement is. Biden is saying right out loud that he is more concerned with the optics of the situation than he is with the suffering of the human beings that he is deporting without so much as a court hearing.
The Release Of Meng Wanzhou's Is A Small But Decisive Victory For China
The U.S. had, via Canada, taken Meng Wanzhou as a hostage. China replicated that by taking two Canadian citizens as hostages, thereby putting the pressure on the weaker power involved. It also stopped imports of Canadian canola and pork. No government will want to repeat the experience of the Canadian one.
The US Space Force Will Wear Battlestar Galactica Uniforms
Orwellian Fare:
Australians Need To Decide If This Is The Kind Of Country We Want To Live In From Now On
How far is too far? Looking at the footage that’s been circulating these past few days, I would say that too far is in our rearview mirror right now. Time to hit reverse and start saying no.
We Won’t Be Free Until Our Minds Are Free
[More] CaitOz Fare:
People Don’t Understand How Unfree We Already Are
The biggest and most widespread blind spot among those who oppose totalitarian control by the powerful is the assumption that it has not already been achieved.
We’ve been so busy watching out for the next overtly totalitarian dictatorship that wants to put the jackboot on our necks we never noticed the covert totalitarians sliding the shackles around our minds.
Everyone thinks about the abusers who beat their spouses, but not the abusers who dominate their spouses’ minds with psychological manipulation.
People assume that they aren’t already behaving exactly how the powerful want them to behave within a civilization whose political, monetary and economic systems are already completely under the control of the powerful.
…
None of the people warning of Orwellian dystopia get it: we’re already there.
…
We are trapped. We are checkmated. At least, as long as our minds continue to operate in a way that can be easily manipulated.
People say, “Why pick on AOC when other lawmakers are way worse?”
They’re not worse, they just perform different functions. The Manchins and Sinemas kill leftward movement openly, the AOCs encourage the left to feed their political energy into a party that’s built to kill leftward movement.
It happens that one of these manipulations is much easier for leftwardy-inclined people to see than the other; it’s easier to recognize Manchin and Sinema-type bullshit than AOC-type bullshit. So you’ll see some factions on the left putting special emphasis on pointing out the one that the general public needs a lot more help recognizing.
Other Quotes of the Week:
Trudeau may be a terrible person, a liar, a poseur and a sociopath, if not worse, but he has a strong survival instinct and knows how to strike a pose. His one professional expertise, drama, (lying and pretense) has carried him through two elections and may, given the low information capacity of the average voter, carry him to a third minority.
Doctorow: FB's mission is to increase the size of the shit-sandwich they can force you to eat before you walk away. But they're not mere sadists: shit-sandwiches have a business model: the more hostages they take, the more they can extract from advertisers - their true customers.
Big Thoughts:
Ian Welsh: The Wages Of Embarrassing Elites Are Death
Everyone remember the Panama papers? A leak of bank records showing that the ultra-rich are hiding massive wealth, tax-free and often breaking the law to do so? A rather weak set of laws designed to allow tax avoidance by rich people, at that. Found out the other day that the reporter who broke the Panama Papers story was killed by a car bomb.
Coincidence, no doubt.
You may recall the Ferguson protests, started after another black man was killed by a cop. They were a big deal.
Since then six of the Ferguson protest leaders have died: two inside burnt cars, three by suicide, one an overdose.
Coincidence, no doubt.
Then there was a high ranked pimp, who flew important men like Bill Clinton and Bill Gates and Prince Andrew in his private jet and provided under-age women for sex. The first time he was indicted he was let off because the prosecutor was told to back off, as he belonged to intelligence. The second time, influence not having worked, he “committed suicide” in prison.
I used to work in life insurance. There’s an adage, backed up by lots of studies, that people who are worth more dead than alive tend to die a lot more than the actuarial tables would suggest for someone of their age and health.
Coincidence, no doubt.
The simplest fact of modern life is elites kill and impoverish other people in order to make money and secure their power. You are seeing it in the pandemic, where Billionaire wealth has spiked 60% and vaccine companies refuse to share their “intellectual property” while planning to sell Covid booster shots in perpetuity. Actually wiping out Covid would close pharma money, but if it stays around, it’s golden.
Meanwhile, all the small and medium businesses closing has lead to a vast buying opportunity for those with lots of money, and private equity is moving big into buying up distressed homes.
It’s just business, baby. Your death, or homelessness, well, it’s someone else’s profit opportunity.
We have the richest wealthy the world has ever seen; even more than the gilded Age. Richer than kings and emperors. They are rich exactly because they hold political power: in the period from 32 to the 70s they lost relative wealth and income, because that’s what government policy was set up to to do.
So they bought up intellectuals like Milton Friedman and politicians like Reagan, Thatcher, Blair, Clinton and Obama, along with tens of thousands of lesser lights. They changed how government was run. It lowered taxes massively, sold off its crown jewels, and got rid of regulations meant to keep wages up while education and housing were cheap.
It’s not that long ago. I remember the last parts of the post-war era, and many people still living remember the 50s and 60s, even as adults.
But that world is long, long dead, and we live in a new one. One where it doesn’t matter if climate change or a pandemic will killing millions or billions. One where lower wages are good, and the Federal Reserve intervenes constantly to lower them, while always making sure the rich never lose everything in a financial collapse.
And in this world, the rich kill and impoverish you for money. Usually they do it in ways they can pretend aren’t about them: policy changes, or increases to insulin prices, but if you really get on their nerves or might even be a real threat, as with our pedophile pimp (and almost certain blackmailer) Jeffrey Epstein, well, people who are worth more dead than alive, they tend to get dead.
Are you worth more dead than alive to some rich person, or some politician in the pay of said rich people?
Satirical Fare:
Pfizer Assures That Vaccine Is Almost As Safe For Kids As COVID
Pics of the Week:
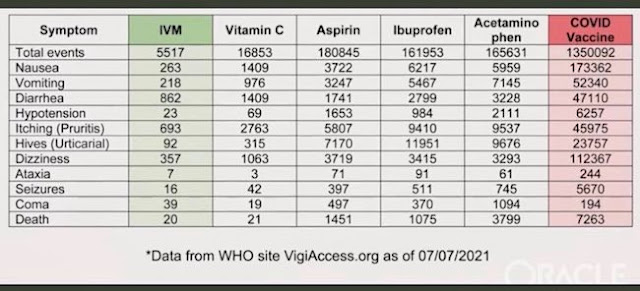


Mathew Crawford: A new hero has emerged. Mostly-retired scientist Ronald Kostoff, PhD, and a highly experienced team, just had their paper published. The appropriate, if understated title of the paper is: Why are we vaccinating children against COVID-19? Let us appreciate his restraint in never using the word "assholes" anywhere in the paper. At the age of 84, he maintains a level of polite discipline in the face of assholes I can scarcely muster on my better days.
COVID Tweets of the Week:
Highly effective home care kits in India & Latin America avg cost $2.65 shows why this hasn’t happened in “developed” world.
Avg vaxx cost $16.25/dose Pfizer, $19.20 Moderna x2 +boosters. Manufacturing cost $2.85/dose.
Recovery w/home care likely immune 4 life w/o side effects.
Kulldorff: By mandating vaccines for those who have had COVID, @NIAIDNews director Anthony Fauci questions natural immunity after COVID disease. That's like having the nation’s lead astronomer question whether the earth is round or flat.
Kory: Uttar Pradesh COVID cases now effectively ZERO given population of 241 million, massive testing, 5% vax. Rivals the historic eradications of smallpox & polio with vaccines, except those were celebrated in all the papers and all the streets… while UP’s IVM strategy.. not a peep
Did they force people who already had Covid to get the vaccine in order to inflate the success rate of the vaccine by embedding natural immunity into the data?
Yes, forcing people out of their jobs and into poverty because of a personal medical decision is wrong, actually.
On the eve of the introduction of medical apartheid in Ontario what may be hardest to deal with is that the large majority —your friends, family, colleagues, strangers—*support* government banning you and so many others from society.
Forgive them, for they know not what they do.
COVID Conspiracy Fare:
10+ Years to Stop the Spread
We’re not getting out of this pandemic anytime soon. The government has no idea what they’re doing, they manipulate the numbers of cases and deaths, they lie to us constantly, they’re rationing therapeutics and they’ve allowed more than a million illegal aliens into the country this year during a pandemic. It’s obvious that the democrats don’t want COVID-19 going anywhere. And who can blame them? It helped them get rid of Trump by cheating in an election and has allowed them to be able to rule over us tyrannically in every facet of government – federal, state, county, city, townships, health departments, school boards, OSHA, licensing boards and more.
Everyone and their brother (and sister) in government has been trying to control what we do and take away our freedoms – presidents, governors, mayors, attorney generals, health directors, and local commissioners. The democrats have also been able to control us with school boards, leftist businesses, social media and the fake news on their side. COVID-19 was a gift to the democrats and it’s a gift that keeps on giving. They have no intention to let it go. At this point, it really doesn’t matter how many vaccines and therapeutics we come up with because we can’t end a pandemic with open borders and a democrat president who ships these people all over the country. So we’re going to have to learn to live with the pandemic for a long long time – and different variants of the virus.
Because of this, I have a kind of apocalyptic prediction that this will end up being an extinction level event. I’m not sure what the timeline is. Five years, ten years, maybe more if we slow it down a bit here and there. But I’m starting to believe that the virus will stop spreading when a large percentage of the people on the planet stop breathing. There are too many leftists around the world keeping this thing going. But the democrats will be okay with that because it means a lot less carbon dioxide being emitted into the air from that breathing. A lot less cows will needed for food, a lot less cars will be driving around and a lot less airplanes will be flying in the skies. So it’s pretty much a winning situation if the virus goes on for a while and destroys a lot of people in its path. The only way the democrats DON’T win is if the virus is beaten. And the democrats NEVER want to lose. Think about that.
GeoPolitical Fare:
Whitney Webb: The Politics of Fear and Self-Preservation
Many of those who have been quick and vocal to point out the lies of the US government when it comes to the invasions of Afghanistan and Iraq and other consequences of the War on Terror have been unable to even consider that the official story of 9/11 may not be legitimate and may indeed have been dealt from the same pack. This may be for a variety of reasons, including a strong desire to not be de-legitimized by their peers as bearers of the “conspiracy theorist” smear and an unwillingness to face a political reality where US government officials may have been complicit in a deadly attack on American soil. In those two examples, however, the failure of such individuals, particularly in media, to even consider that there may be more to the story boils down to a desire for self-preservation in the case of the former and preservation of a particular worldview in the case of the latter.
Yet, in both cases, the casualty is the truth and the cause is cowardice. By failing as a society to thoroughly examine the events of 9/11 and why those events occurred, the American public has shown the powers that be that their desire to preserve a “safe” worldview — and to preserve their own careers, in the case of certain professional classes — is enough to keep people from questioning world-altering events when they emerge. Those powers are well aware of this refusal and have been using it to their advantage ever since. Today, with the COVID-19 crisis still dragging on, we are similarly immersed in a situation where nuance and facts are being cast aside, militantly in some cases, in favor of the establishment narrative. Is everyone who chooses not to take this particular vaccine a “conspiracy theorist” and “anti-vaxxer”?
Does it really make sense to so dramatically divide the public into groups of vaccinated and unvaccinated through a new ID system when the vaccine claims to reduce the severity of illness but not to stop disease transmission? Should those that question the motivation of politicians, powerful pharmaceutical corporations and mainstream media “experts” be censored from expressing those views online? You do not need to agree with those who hold such views, but what is wrong with hearing what they have to say and debating their evidence with your own?
We are losing the ability to have rational public discourse about these issues — and losing it swiftly, at a speed comparable to what took place in the aftermath of 9/11, when questioning the motives of the Bush administration, US intelligence agencies and other groups, as well as their proposed responses and “solutions,” was deemed “unpatriotic” and even “treasonous” by some. Calls were made to strip an entire class of Americans of their freedom for merely sharing the same ethno-religious identities as those we were told attacked us, and many went along with it. Freedom became treated as a privilege only for certain groups, not as a right, and this insidious fallacy has reared its head yet again in recent months in relation to the COVID-19 vaccine debate and also the war on domestic terror.
Greenwald: New Proof Emerges of the Biden Family Emails: a Definitive Account of the CIA/Media/BigTech Fraud
An axis of the CIA, Big Tech and the DNC-allied wing of the corporate media spread an absolute lie in the weeks before the 2020 election. We now have definitive proof.
The Horses' Asses of the Apocalypse
The worst thing about the atrocious treatment of the Haitian refugees for Biden, though, is that the photographic evidence of systemic US cruelty - rather than the cruelty itself - is an embarrassment to him personally. It makes him look bad, especially when the images were released just as he was belligerently touting American peace, love, democracy and freedom to the rest of the world at the United Nations' annual summit this week.
“It’s an embarrassment. It’s beyond an embarrassment. It’s dangerous, it’s wrong, it sends the wrong message around the world or sends the wrong message at home," he fumed, ending his spiel with the obligatory "It's not who we are!"
It's hard emphasize enough just how craven and downright psychopathic this statement is. Biden is saying right out loud that he is more concerned with the optics of the situation than he is with the suffering of the human beings that he is deporting without so much as a court hearing.
The Release Of Meng Wanzhou's Is A Small But Decisive Victory For China
The U.S. had, via Canada, taken Meng Wanzhou as a hostage. China replicated that by taking two Canadian citizens as hostages, thereby putting the pressure on the weaker power involved. It also stopped imports of Canadian canola and pork. No government will want to repeat the experience of the Canadian one.
The US Space Force Will Wear Battlestar Galactica Uniforms
Orwellian Fare:
Australians Need To Decide If This Is The Kind Of Country We Want To Live In From Now On
How far is too far? Looking at the footage that’s been circulating these past few days, I would say that too far is in our rearview mirror right now. Time to hit reverse and start saying no.
We Won’t Be Free Until Our Minds Are Free
[More] CaitOz Fare:
People Don’t Understand How Unfree We Already Are
The biggest and most widespread blind spot among those who oppose totalitarian control by the powerful is the assumption that it has not already been achieved.
We’ve been so busy watching out for the next overtly totalitarian dictatorship that wants to put the jackboot on our necks we never noticed the covert totalitarians sliding the shackles around our minds.
Everyone thinks about the abusers who beat their spouses, but not the abusers who dominate their spouses’ minds with psychological manipulation.
People assume that they aren’t already behaving exactly how the powerful want them to behave within a civilization whose political, monetary and economic systems are already completely under the control of the powerful.
…
None of the people warning of Orwellian dystopia get it: we’re already there.
…
We are trapped. We are checkmated. At least, as long as our minds continue to operate in a way that can be easily manipulated.
People say, “Why pick on AOC when other lawmakers are way worse?”
They’re not worse, they just perform different functions. The Manchins and Sinemas kill leftward movement openly, the AOCs encourage the left to feed their political energy into a party that’s built to kill leftward movement.
It happens that one of these manipulations is much easier for leftwardy-inclined people to see than the other; it’s easier to recognize Manchin and Sinema-type bullshit than AOC-type bullshit. So you’ll see some factions on the left putting special emphasis on pointing out the one that the general public needs a lot more help recognizing.
Other Quotes of the Week:
Trudeau may be a terrible person, a liar, a poseur and a sociopath, if not worse, but he has a strong survival instinct and knows how to strike a pose. His one professional expertise, drama, (lying and pretense) has carried him through two elections and may, given the low information capacity of the average voter, carry him to a third minority.
Doctorow: FB's mission is to increase the size of the shit-sandwich they can force you to eat before you walk away. But they're not mere sadists: shit-sandwiches have a business model: the more hostages they take, the more they can extract from advertisers - their true customers.
Big Thoughts:
Ian Welsh: The Wages Of Embarrassing Elites Are Death
Everyone remember the Panama papers? A leak of bank records showing that the ultra-rich are hiding massive wealth, tax-free and often breaking the law to do so? A rather weak set of laws designed to allow tax avoidance by rich people, at that. Found out the other day that the reporter who broke the Panama Papers story was killed by a car bomb.
Coincidence, no doubt.
You may recall the Ferguson protests, started after another black man was killed by a cop. They were a big deal.
Since then six of the Ferguson protest leaders have died: two inside burnt cars, three by suicide, one an overdose.
Coincidence, no doubt.
Then there was a high ranked pimp, who flew important men like Bill Clinton and Bill Gates and Prince Andrew in his private jet and provided under-age women for sex. The first time he was indicted he was let off because the prosecutor was told to back off, as he belonged to intelligence. The second time, influence not having worked, he “committed suicide” in prison.
I used to work in life insurance. There’s an adage, backed up by lots of studies, that people who are worth more dead than alive tend to die a lot more than the actuarial tables would suggest for someone of their age and health.
Coincidence, no doubt.
The simplest fact of modern life is elites kill and impoverish other people in order to make money and secure their power. You are seeing it in the pandemic, where Billionaire wealth has spiked 60% and vaccine companies refuse to share their “intellectual property” while planning to sell Covid booster shots in perpetuity. Actually wiping out Covid would close pharma money, but if it stays around, it’s golden.
Meanwhile, all the small and medium businesses closing has lead to a vast buying opportunity for those with lots of money, and private equity is moving big into buying up distressed homes.
It’s just business, baby. Your death, or homelessness, well, it’s someone else’s profit opportunity.
We have the richest wealthy the world has ever seen; even more than the gilded Age. Richer than kings and emperors. They are rich exactly because they hold political power: in the period from 32 to the 70s they lost relative wealth and income, because that’s what government policy was set up to to do.
So they bought up intellectuals like Milton Friedman and politicians like Reagan, Thatcher, Blair, Clinton and Obama, along with tens of thousands of lesser lights. They changed how government was run. It lowered taxes massively, sold off its crown jewels, and got rid of regulations meant to keep wages up while education and housing were cheap.
It’s not that long ago. I remember the last parts of the post-war era, and many people still living remember the 50s and 60s, even as adults.
But that world is long, long dead, and we live in a new one. One where it doesn’t matter if climate change or a pandemic will killing millions or billions. One where lower wages are good, and the Federal Reserve intervenes constantly to lower them, while always making sure the rich never lose everything in a financial collapse.
And in this world, the rich kill and impoverish you for money. Usually they do it in ways they can pretend aren’t about them: policy changes, or increases to insulin prices, but if you really get on their nerves or might even be a real threat, as with our pedophile pimp (and almost certain blackmailer) Jeffrey Epstein, well, people who are worth more dead than alive, they tend to get dead.
Are you worth more dead than alive to some rich person, or some politician in the pay of said rich people?
Satirical Fare:
Pfizer Assures That Vaccine Is Almost As Safe For Kids As COVID
Pics of the Week:


